

Abstract
Aim
This paper, the second of two, aims to provide information to help pharmacists discuss economically important choices about which statin to use with prescribers. NICE guidelines recommend a specific first-choice statin and a dose for some indications, but not for others.
Design
The paper highlights three relevant questions, suggests responses to them and suggests first- or second-line statin choices informed by those responses.
Content
Included are Panels showing the cost of the various statins and the mean percentage reduction in LDL cholesterol achieved by simvastatin, atorvastatin and rosuvastatin. The paper outlines three questions that are relevant to choices when greater LDL cholesterol reduction than is achievable with simvastatin 40mg daily is indicated, and provides suggested responses to those questions and a Table of suggested statin choices informed by those responses.
Three clinical guidelines from the National Institute for Health and Clinical Excellence (NICE) cover statin use in some detail: there are guidelines on lipid modification,1 type 2 diabetes2 and on familial hypercholesterolaemia.3
The guidelines recommend a specific first-choice statin and dose for some indications — such as primary prevention in the absence of familial hypercholesterolaemia — but not for others, such as acute coronary syndrome, where the recommendation is to offer a higher intensity statin, with higher intensity statin defined as one used in doses that produce greater cholesterol lowering than simvastatin 40mg. For some indications the guidelines include ezetimibe among options to be considered.
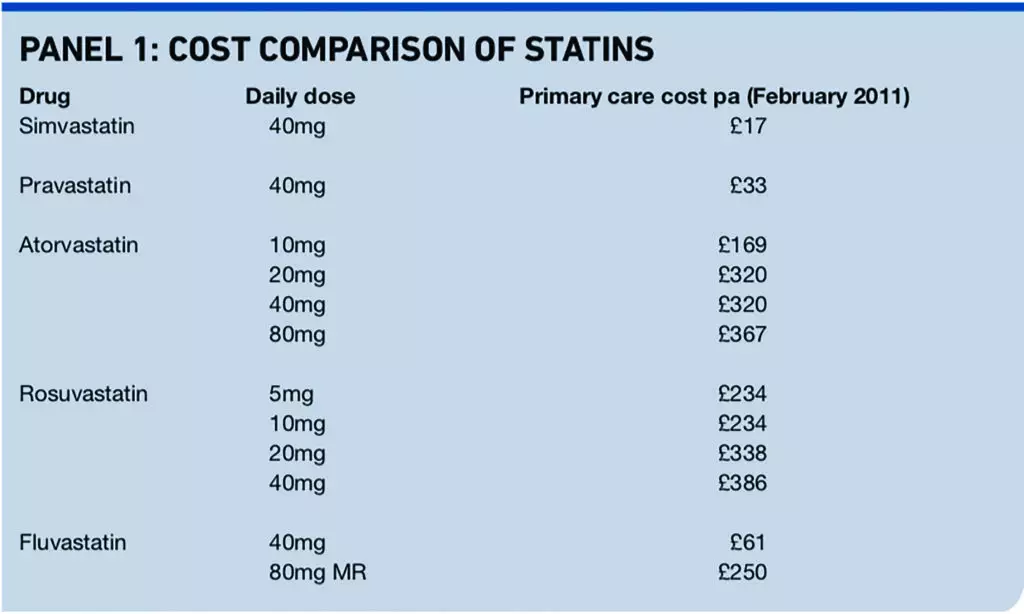
The choice of statin is important, in part because of the large difference in the price of low-cost generic statins compared with statins protected by patent or supplementary protection certificate (See Panel 1).
This paper highlights three relevant questions, suggests responses to them and then suggests first- or second-line statin choices informed by the responses.
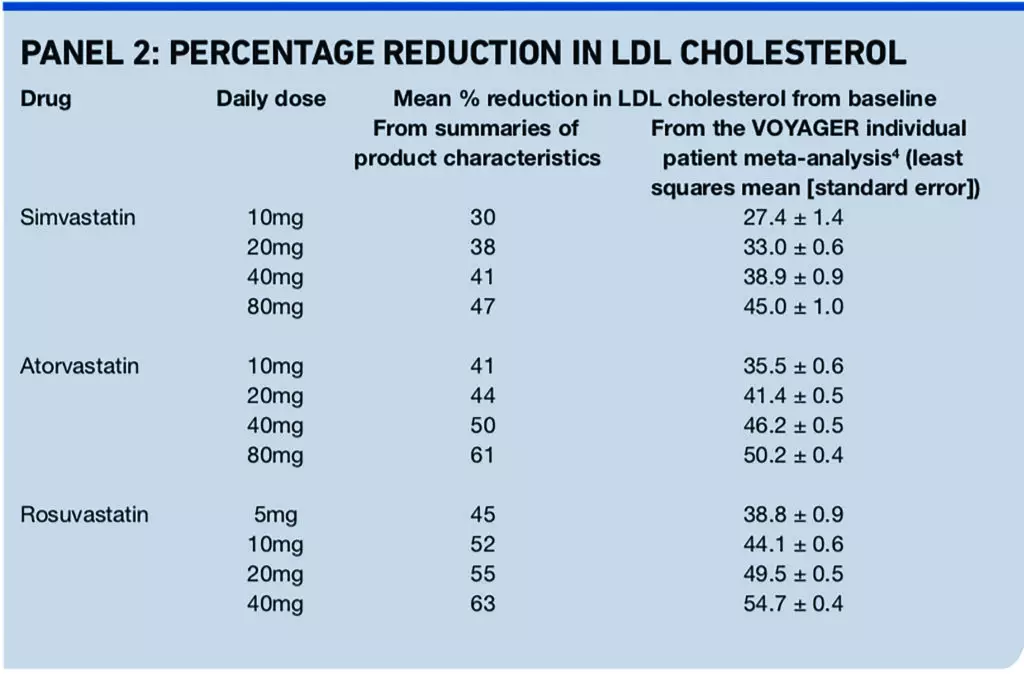
Panel 2 shows the percentage reduction in LDL cholesterol achieved by simvastatin and the more potent statins atorvastatin and rosuvastatin.
Questions and suggested responses
Question 1
In some circumstances the guidelines issued by NICE suggest considering increasing the dose of simvastatin to 80mg daily. These guidelines were published before the recent warning from the Medicines and Healthcare products Regulatory Agency about increased risk of myopathy associated with 80mg simvastatin5 and the finding by the Cholesterol Treatment Trialists’ Collaboration that all the observed excess of rhabdomyolysis with more intensive statin therapy occurred in trials of simvastatin 80mg versus 20mg daily.6 Given this, is it still reasonable to increase a patient’s simvastatin dose to 80mg daily rather than using a more potent statin?
Suggested response
It is best to avoid new prescriptions for simvastatin 80mg daily. If greater LDL cholesterol reduction than is achievable with simvastatin 40mg daily is indicated, it is preferable to use a more potent statin.
Question 2
If the prescriber decides not to write new prescriptions for simvastatin 80mg daily, which of the newer, more potent statins should be used instead?
Suggested response
Factors to take into account include:
- The Cholesterol Treatment Trialists’ Collaboration finding that each 1.0mmol/L reduction in LDL cholesterol reduces the annual rate of major vascular events by just over a fifth6
- The patient’s baseline LDL cholesterol and the mean percentage reductions achieved by the various doses of atorvastatin and rosuvastatin (for example, Panel 2 shows that the mean reduction with rosuvastatin 20mg is around 3.3 to 5 per cent greater than the reduction with atorvastatin 40mg daily, so for a patient with baseline LDL cholesterol of 5.0mmol/L using rosuvastatin 20mg rather than atorvastatin 40mg might reduce LDL cholesterol by around 0.25mmol/L more)
- The British National Formulary statement that the dose of rosuvastatin should only be increased to 40mg daily under specialist supervision
- Current prices
- The November 2011 expiry of the UK Supplementary Protection Certificate for atorvastatin (cheaper generics should then appear, although it is not possible to say how rapidly the Drug Tariff price would fall)
- How likely it is that the patient could and would be switched from rosuvastatin to atorvastatin when the Drug Tariff price of atorvastatin falls significantly
Question 3
How does ezetimibe, another LDL cholesterol lowering drug, fit in?
Suggested response
NICE guidance on ezetimibe for primary hypercholesterolaemia is available at http://guidance.nice.org.uk/TA132/Guidance/Recommendation.
A recent systematic review compared the benefits and harms of high-dose statin monotherapy with those of combination therapy (statin plus lipid modifying drugs other than statins) in adults at high risk of coronary disease.7 No trials compared the effect of combination therapy versus high- dose statin monotherapy on the incidence of myocardial infarction, stroke, or revascularisation procedures.
The Drug and Therapeutics Bulletin recently questioned whether adding ezetimibe to statin treatment is a cost-effective or outcome-based intervention.8 There are no published trials to show it reduces mortality or morbidity. The DTB said: “Since it is proving increasingly expensive for the NHS, prescribers should ask why they are using [ezetimibe].”8
Ezetimibe 10mg/day costs £342 a year. The ezetimibe 10mg plus simvastatin 40mg combination product costs £507 a year.
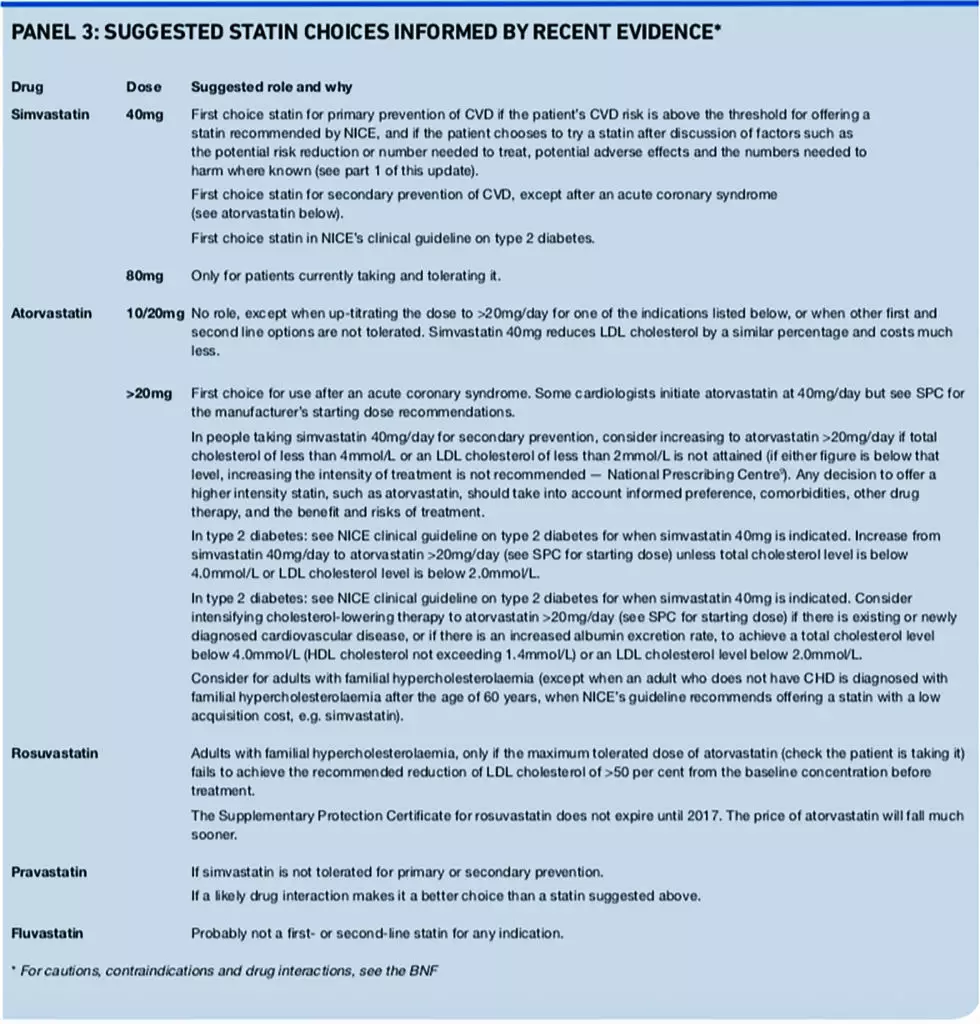
The suggestions in Panel 3 below assume:
- The prescriber agrees that it is best to avoid new prescriptions for simvastatin 80mg daily
- Atorvastatin is favoured over rosuvastatin because prices of the former are likely to fall sooner
- It is generally best to use a statin alone, when not contraindicated and when tolerated, rather than adding ezetimibe
- The suggested drug is tolerated
Choosing which statin to use remains economically important. The financial challenge currently facing the NHS makes it particularly important not to use higher priced statins for indications for which NICE’s guidance recommends low cost simvastatin or pravastatin.
About the author
Chris Corfield is chief pharmacist at NHS Hammersmith and Fulham (email Christopher.Corfield@hf-pct.nhs.uk)
References
- NICE clinical guideline 67. Lipid modification. Cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease. London: NICE, 2008.
- NICE clinical guideline 87. Type 2 diabetes. The management of type 2 diabetes. London: NICE, 2009.
- NICE clinical guideline 71. Familial hypercholesterolaemia. Identification and management of familial hypercholesterolaemia. London: NICE, 2008.
- Nicholls S, Brandrup-Wognsen G, Palmer M, Barter P. Meta-analysis of comparative efficacy of increasing dose of atorvastatin versus rosuvastatin versus simvastatin on lowering levels of atherogenic lipids (from VOYAGER). American Journal of Cardiology 2010;105:69–76.
- Medicines and Healthcare products Regulatory Agency. Simvastatin: increased risk of myopathy at high dose (80mg). Drug Safety Update 2010;3(10):7.
- Cholesterol Treatment Trialists’ (CTT) Collaboration. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants 8 in 26 randomised trials. Lancet 2010;376:1670–81.
- Sharma M, Ansari M, Abou-Setta A, Soares-Weiser K, Ooi T, Sears M et al. Systematic review: comparative effectiveness and harms of combination therapy and monotherapy for dyslipidemia. Annals of Internal Medicine 2009;151:622–30.
- Money, money, money. Drug and Therapeutics Bulletin 2010;48:73.
- National Prescribing Centre. What is the place in therapy of simvastatin 80mg in the light of recent MHRA guidance? MeReC Monthly 2010;(July):1–2.


